Headline News
Understanding Subdural Collections In Pediatric Abusive Head Trauma
December 13, 2021
Understanding Subdural Collections In Pediatric Abusive Head Trauma
Wittschieber D, Karger B, Pfeiffer H, Hahnemann ML
http://www.ajnr.org/content/40/3/388.long
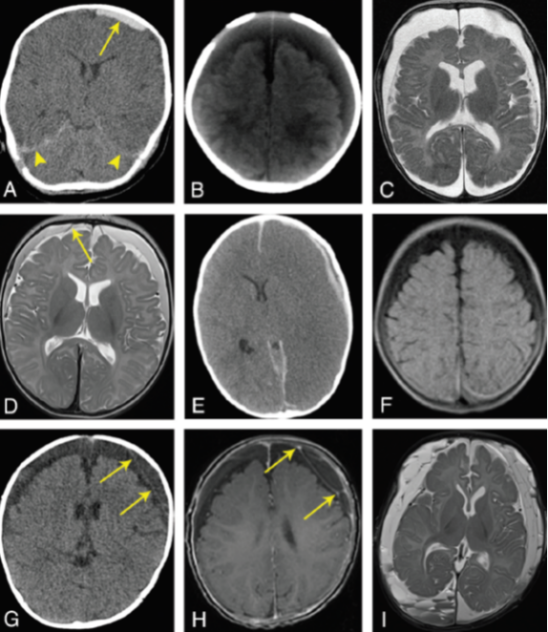
Subdural collections (SDC) are the most frequently encountered neuroimaging finding in abusive head trauma (AHT). Wittschieber et al. describe the pathophysiology of SDCs and help us understand the limitations of neuroimaging for precise dating of SDCs. Six types of SDCs are described: Subdural hematoma (SDH), subdural hygroma (SDHy), subdural hematohygroma (SDHHy), chronic subdural hematoma (cSDH), subdural effusion, and subdural empyema; the latter two are the sequelae/complications of meningitis or sinusitis.
In the context of AHT, the authors highlight the following concepts regarding SDC’s:
- Shearing and rotational forces from AHT may cause bridging vein (BV) rupture, resulting in extra-axial hemorrhage, predominantly within the subarachnoid (SAH) and subdural spaces (SDH). The susceptibility of BVs to rupture is related to the decreased vessel wall thickness of the segments that penetrate the dura mater and lack the additional surrounding connective tissue.
- Arachnoid tears may happen concomitantly during the shearing injury, resulting in transfer of CSF into the subdural space and formation of SDHys or SDHHys.
- Mixed-density SDCs should not be misinterpreted as a mixture of “new” and “old” hemorrhage. They can be seen in the context of at least four different scenarios, three of which may be the result of a single traumatic event, including mixture of unclotted and clotted blood, compacted clot with serum separation, and BV injury with concomitant arachnoid tear and CSF influx.
- In cSDH, an outer subdural neomembrane forms and is followed by the formation of an inner subdural neomembrane. These neomembranes are highly vascularized with fragile blood vessels that may leak blood, proteins, and fluid into the cSDH, possibly expanding it. Formation of septations within the cSDH, a consequence of rebleeding, may result in multiple chambers within the cSDH that contain fluid-fluid levels.
- Acute rebleeding in a cSDH resulting in a mixed-density SDC is not typically associated with the acute symptomatology of abusive head trauma.
- Reliable aging of hypodense SDCs is impossible! Unclotted blood, clotted blood in the setting of anemia, CSF accumulation into a SDH, and lysis of erythrocytes may all cause a hypodense SDC in the acute post-traumatic setting and should not be misinterpreted as a cSDH.
- The most important diagnostic imaging finding in diagnosing an aging SDH, is the visualization of neomembranes, septations, or chamber formations. Neomembranes take 2-4 weeks to appear on imaging.
- The authors propose a “minimum age concept” for SDCs rather than precise dating. For instance, the development of a chronic subdural hematoma takes at least 2 weeks.
- Considering that precise dating is impossible, serial neuroimaging may help correct age estimation of SDCs.

Melike Guryildirim, MD
The Johns Hopkins Hospital